Question:
A patient with a pituitary tumor that overproduced growth hormone underwent surgical removal of the tumor. The resection was found to be incomplete. What is the first-line treatment for this patient?
A patient with a pituitary tumor that overproduced growth hormone underwent surgical removal of the tumor. The resection was found to be incomplete. What is the first-line treatment for this patient?
Updated On: Jun 18, 2025
- Leuprolide
- Goserelin
- Nafarelin
- Octreotide
Show Solution
Verified By Collegedunia
The Correct Option is D
Solution and Explanation
The patient in question has a pituitary tumor leading to excess production of growth hormone. After surgical removal, it has been determined that the resection was incomplete, indicating residual tumor activity that requires further intervention. In such scenarios, the first-line treatment to manage excess growth hormone production is the use of somatostatin analogs. Octreotide is a synthetic somatostatin analog that acts by inhibiting the release of growth hormone from the pituitary gland. It is specifically effective due to its ability to reduce growth hormone levels and is commonly used when surgery does not completely remove the tumor. Thus, given the options:
| Leuprolide | A gonadotropin-releasing hormone agonist, not typically used for growth hormone management. |
| Goserelin | Another gonadotropin-releasing hormone agonist with uses similar to Leuprolide. |
| Nafarelin | Similar in function to the above but not standard for this condition. |
| Octreotide | Correct choice, a somatostatin analog effective in reducing growth hormone levels. |
Thus, for this patient, Octreotide is the appropriate first-line treatment after incomplete surgical resection of a growth hormone-secreting pituitary tumor.
Was this answer helpful?
0
0
Top NEET PG Anatomy Questions
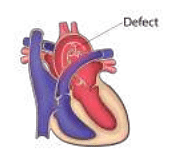
- A defect in which of the following forms the structure marked below?

- A student had his jaw locked while yawning. Which of the following muscles is attached to the articular disc of the temporomandibular joint?
- The given histology image is of ?

- A defect in which of the following aortic arches causes the defect shown in the image?
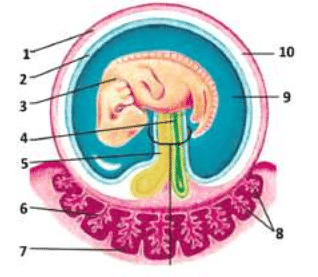
- Which of the following structures develops from the structure marked 4?
View More Questions
Top NEET PG Endocrine Glands Questions
- Hormone predominately secreted after 14 day on endometrium is?
- Calcitonin levels increased in:
- C-peptide seen in?
- Testosterone secreted by,
- Vasopressin acts through which channels in collecting duct?
View More Questions
Top NEET PG Questions
- A patient hailing from Delhi presents with fever, arthralgia, and extensive petechial rash for 3 days. Lab investigations revealed a hemoglobin of 9 g/ dL, a white blood cell count of 9000 cells/mm3, a platelet count of 20000 cells/mm3, and a prolonged bleeding time. The clotting time was normal. What is the most likely diagnosis?
- Which of the following statements is true about Trichomonas vaginalis?
- A lady from West Rajasthan presented with an ulcer surrounded by erythema on the right leg. Microscopy of the biopsy from the edge of the ulcer showed organisms with dark staining nuclei and kinetoplast. What is the most likely causative agent?
- A child presents with a fever and a rash. Urine examination showed cells with owl's eye appearance. What is the most likely diagnosis?
- Infection with Clonorchis sinensis is associated with an increased risk of__?
View More Questions